What We Offer
Multifetal Pregnancy Management
Since the 1980s our program has been considered the leading provider of multiple pregnancy management by fetal reduction. We published the first and most of the leading-edge papers on the subject.
Over the past three decades, the number of twin births has more than tripled in the United States. There has been a 13-fold increase in triplets, the rate of quadruplets has increased 100 times, and there had been a 1,000-fold increase in quintuplets. Over the past several years, with better control of infertility treatments, the number of very high order multiples has come down considerably, but twins remain many times natural expectations. For patients with multiple pregnancies, the risks of loss, prematurity, congenital anomalies, and poor neonatal outcomes are dramatically higher than for singletons. For twins, loss rates are more than double singleton rates, and cerebral palsy is 5 times as high. For triplets, loss rates are 10 times as high as a singleton, and cerebral palsy is 15 times higher. For even higher numbers, the statistics are even worse.
Genetic risks are multiplied by the number of fetuses. For example, for a 35 year old with triplets, the risk of a chromosome abnormality at birth would be 1/190 for a singleton but is 3/190 or about 1/65 for one of fraternal triplets. That is comparable to the risk of a 40 year old. Thus, we prefer to perform genetic testing by CVS prior to reduction to maximize the likelihood of a healthy family. We typically see patients for multifetal pregnancy reduction (MFPR) now also interchangeably termed fetal reduction (FR) at about 12 weeks. For the 85% of our patients who are also having CVS, the procedures are done usually over two days.
With the development of microarray analysis as part of the CVS results, patients have options.
- For most of our patients coming from out of town, they still prefer to perform the reduction based upon the FISH results – so that everything can be done in one trip.
- For local patients, most are waiting for the microarray results to come back to have the most complete information before FR.
We sometimes perform the reductions in multiple steps. For example, for a patient wanting to go from triplets to a singleton, we typically will do CVS on all 3 triplets, reduce to twins based upon the FISH, wait for the microarray and then reduce to a singleton.
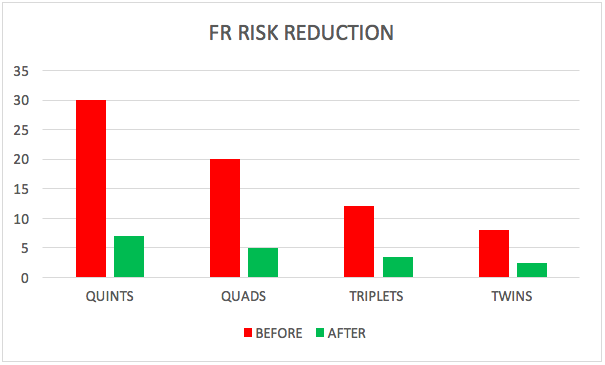
Over the past 35 years, Dr. Evans has been a pioneer in the practice of MFPR having performed thousands of such procedures for patients starting with between 2 to as many as 12 fetuses. The procedure has been demonstrated to be a safe way to significantly reduce the risks of multiple pregnancies. Patients with triplets or higher have their risks cut by more than half by reducing to twins. For twins, the risks of pregnancy loss and prematurity can be further cut by reducing to a singleton.
In deciding which fetuses to keep or to reduce, we prioritize decisions by:
1. Do we find a problem.
2. Are we still suspicious about the health and prognosis for a fetus
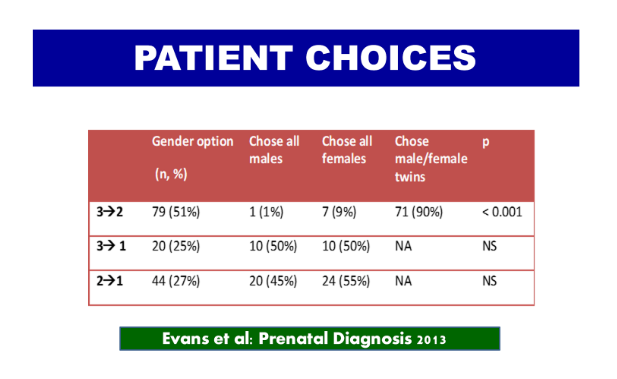
3. If nothing else matters and we have done CVS, we can then consider gender. We only adopted this position when our data showed that gender preference is overall now equal, i.e. females are just as preferred as males.
When we first developed FR in the 1980s and there were very little data, we still felt it important to create ethical guidelines as to how to proceed. Dr. Evans worked with Dr. John Fletcher (head of the bioethics program at the National Institute of Health), we concluded that we should not reduce below twins. This conclusion was based upon the facts that:
- Every obstetrician can handle twins.
- The risk of twins, while higher than a singleton, was “reasonable” given the poor quality of infertility treatments in the 1980s.
- The outcomes with twins are far higher than previously appreciated.
- There always were exceptions: e.g. the woman is a dwarf, has cardiac disease, has a uterine, or fetal abnormality. The data in these cases have shown, that even for the woman who starts with twins, if one defines “success” as healthy mother and healthy family, pregnancy outcome is improved by 2 to 1.
If one believes that 1 to 0 is ever acceptable (i.e., the right to terminate a pregnancy), then why not 2 to 1.
As fertility treatments have improved and the incidence of the higher order number multiples has been considerably reduced, nearly half of our FR cases are now 2 to 1. Virtually all of such patients have CVS before FR.
For more information, please see the attached publications that provide much more detail.
- Evans MI, Andriole SA, Britt DW: Fetal Reduction – 25 years’ experience.
- Evans MI, Rosner M, Andriole S, Alkalay A, Gebb J, Britt DW: Evolution of gender options in multiple pregnancy management.
- Multifetal Pregnancy Reduction: Evolution of the Ethical Arguments (By Mark I. Evans, M.D., and David W. Britt, Ph.D)
- The Truth About Multiples (By Mark I. Evans, M.D.)
Subnavigation
Evans Pioneer Award Lecture

-
Quick Contact Info
Dr. Mark I. Evans (MD PLLC)
Phone: 212.288.1422
Fax: 212.879.2606
Email: Evans@CompreGen.com
131 E 65TH ST
NEW YORK NY 10065